
Article by Vivek Radhakrishnan
🩺 Why do we need Intestinal Tissue Engineering?
The intestines aren’t just a tubular organ critical for digestion, but a dynamic multifunctional organ at the epicenter of immune regulation, nutrient absorption and microbial niche management. It has also been associated to manage mental health via the bidirectional gut brain axis. The Intestines, infamously known as “The Gut” has been a topic of discussion from ages, right from ancient philosophies that hypothesize the gut to be the “Second Brain” to modern wellness trends that have been obsessing over prebiotics and probiotics. It has been a constant topic of conversation and debate due to the outsized role it plays in our survival and quality of life.
But what happens when this essential organ fails?
Thousands of children and adults suffer from Intestinal failure caused by Short Bowel Syndrome (SBS), a complication of necrotizing enterocolitis (NEC), or intestinal atresia or intestinal volvulus. To put things into perspective, each year in the US alone over 1000 infants are born with intestinal failure, with approximately 35% due to necrotizing enterocolitis, 20% attributed to complicated meconium ileus, 12.5% to gastroschisis,10 % to intestinal atresia and 10% to volvulus [1]. Globally, NEC – inflammation and death of intestinal tissue – affects 7-10 % of premature infants with a mortality rate of 50% in severe cases [2]. Given that preterm birth affects ~11% of births worldwide, the burden is significant.
The current primary treatment involves surgical resection of dead tissues, allowing native intestines to further develop and takeover dead tissue. This is supplemented by long term parental nutrition, which is associated with a myriad of serious complications. When the intestines fail to regenerate, there are surgical options available for improving intestinal length but used as a last resort when intestines are severely dilated. When regeneration fails entirely, short bowel transplantation serves as the final treatment option. Transplantation are significantly hampered by organ scarcity, immunosuppressive risk and poor long term survival rates – approximately 43% at 10 years [3]. This clinical bottleneck calls for innovative and transformative solution.
This is where the field of bioengineering steps in—with a interesting idea:
“Can we engineer and build an artificial intestine that recapitulates the native architecture, and functions of the gut to serve as a temporizing intestine – until native bowel adaptation occurs?”
This innovation of artificial intestine could offer personalized immunocompatabile bridge to enteral nutrition, absorbing nutrients and serving the functions of intestines until the host regenerates the intestine, rather than serving as a permanent replacement.
🏗️ How do you build the intestines?
This mammoth task of engineering an artificial intestine was undertaken in the Hackam Lab and led by M R Ladd. The group developed and demonstrated designing a scaffold using a novel fabrication method resulting in an architecture and tensile properties that resembled the native intestine. The scaffold aimed to have a controlled degradation rate, excellent biocompatibility and the capacity to support intestinal stem cells that could recruit host cells and form intestinal tissue in vivo.
The scaffold was made from poly (glycerol sebacate) (PGS). A PMMA template containing villi depressions of 500 um was created by laser ablation and a PDMS mold replicating the villus impressions was created. An agarose replica mold was created by using 3% agarose over the PDMS mold to form a hydrogen replica. This acts as a sacrificial material thereby eliminating the need for applying stress or force during removal of mold and provide a physiologically mild environment for subsequent cell culture.
Polymer solution was poured and fabricated using a modified porogen leaching/thermal induced phase separation technique. The polymer was molded in two separate layers, the base layer containing 30% PGS, large porogen (Sodium Bicarbonate), 2% MDI (crosslinker) and the villus layer containing 30% PGS with a small porogen and 6% MDI. The was villus layer was first poured and subjected to vacuum to ensure complete polymer infiltration of the villus depressions and then the base layer such that at the end of fabrication, a continuous material was created.
The scaffold was coated with collagen-I and seeded with intestinal enteroids. The seeded scaffold was implanted at the mouse omentum to evaluate the immunological response, degradation of the graft and tissue formation in-vivo.
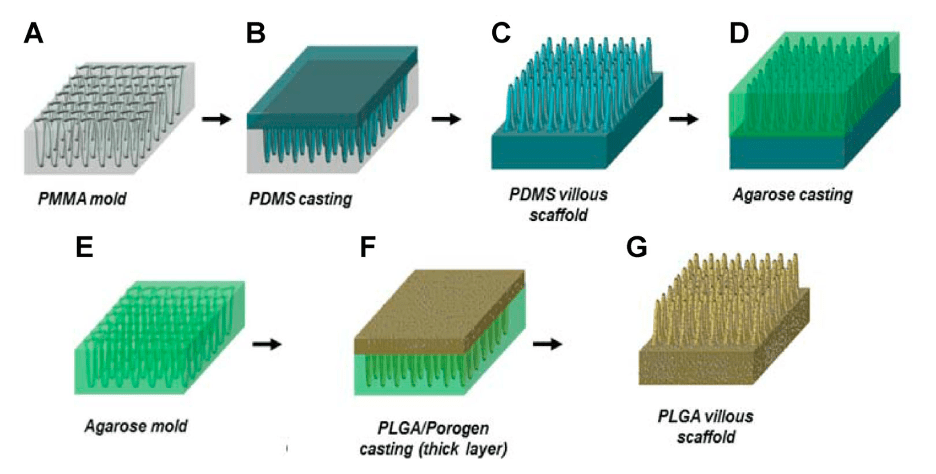
Figure 1: Schematic representation of scaffold fabrication. Current image shows for PLGA scaffold, but the study utilized PGS as scaffolding material [6]
📊 What did the research find?
🧱 Structural Mimicry
- The fabrication method was faithfully able to replicate the intricate architecture of the native intestine with villi dimensions of 647 ± 241 µm diameter, villus height of 340 ± 29.5 µm, and a spacing of 69.5 ± 11 µm, confirmed by SEM.
- The PGS scaffolds maintained their structure during in vitro exposure to cell media, media with digestive enzymes, or when seeded with intestinal stem cells over 6 weeks.
- The stress-strain curves of the material were different than that of native intestines but of same order of magnitude, with E of 5.60 ± 5.05 MPa, and a maximum load of 3.19 ± 1.3 N.
- The PGS scaffolds did possess similar properties such as rollability, held sutures well, and easy to handle thereby mimicking the biomechanical properties.
🧬 Biological Mimicry
- The scaffolds were cytocompatible and accommodated intestinal stem cells well without any morphological change this was demonstrated via MTT assay upon culturing Caco-2 cells and intestinal enteroids transfected with GFP.
- The cells were able to attach to the villi and occasionally span across the inter-villus space, wrapping around the villi and often capping villi. Fewer cells penetrated towards the base than expected. Hence an uneven distribution.
⚙️ Functional Capability
- The scaffold-maintained structure upon omental implantation, without any changes to the villi structure and thickness of scaffold over a 12-week time period.
- In many samples, there was significant amount of tissue deposition on the top of the scaffolds and some areas the tissue nearly reached the base of the villi.
- The PGS scaffolds were well tolerated immunologically with presence of low levels of local inflammation, immune cell infiltrations and fibrosis.
- The scaffolds failed to regenerate tissue and didn’t demonstrate significant tissue ingrowth, indicating the scaffolds inability to recruit host mechanisms for tissue regeneration.
- The limited tissue ingrowth when characterized was absent for intestinal tissue markers, enteric nervous system, mesenchymal stem cells and the scaffold failed to even retain the GFP enteroids seeded.
- The scaffolds thus failed to produce intestinal tissue in-vivo.
- No nutrient absorption or epithelial barrier assays were conducted, highlighting the scaffold’s lack of validated functionality.
| Property | Native Intestine | Engineered Scaffold (PGS) |
| Villus Height | ~500 µm | 340 ± 29.5 µm |
| Villus Diameter | ~700 µm | 647 ± 241 µm |
| Villus Spacing | ~100 µm | 69.5 ± 11 µm |
| Young’s Modulus | 1–6 MPa | 5.60 ± 5.05 MPa |
| Porosity | ~70% | 67% |
| In Vivo Tissue Formation | Present | Minimal/Absent |
| Immune Response | Low (if native) | Low |
| Structural Stability (12 wk) | Maintained | Maintained |

Figure 2: integrity, cellular compatibility, and in vivo performance of the PGS-based artificial intestinal scaffold.
⚠️ What are the limitations and what is next?
The scaffold created did an amazing job at recapitulating the native intestine architecture, and biomechanical properties albeit failed to produce intestinal tissue in-vivo.
- Pore size and connectivity
The scaffold was 67% porous and yet failed to achieve cell infiltration, epithelialization and tissue organization to an acceptable level. This is a critical factor to consider while designing a scaffold, the pore size dictates the type of cell infiltrating and its organization within the scaffold. The pores must also be well connected to help achieve continuous vascularization and epithelialization. This can be further improved by increasing the porogen concentration and using other methods of drying such as lyophilization to form controlled pore sizes.
- Seeding Distribution
The scaffold upon seeding failed to achieve an even distribution of enteroids and had the cells occupy only the villi sections, this coupled with an uneven spatiotemporal scaffold degradation potentially hindered the pace and formation of tissue infiltration. This can be rectified by either coating the scaffold with Matrigel prior seeding and seeding the enteroids on the Matrigel or by using a bioreactor to achieve a continuous culture. A bioreactor could significantly improve the culture and seeding efficiency. The cells could also have enough time to mature prior implantation, this could enhance the cell attachment, distribution and greater differentiation. When coupled with mechanical cues that resemble peristalsis, the cells could better mature and orient themselves into villus-base compartments and achieve greater resemblance to native intestine in-terms of cytoarchitecture. Electrical stimuli when provided may also aid in enteric nervous system differentiation from the stem cell.
- Functional Maturity
Functionally, engineered scaffold lacked critical physiological features such as crypt-villus compartmentalization, peristalsis and absorption capacity with no functional assays performed. Functional assays such as a nutrient absorption or barrier integrity could fortify the constructs functionality.
- Implantation Site
The scaffolds were tested in-vivo by implantation at the omentum, this may not be the apt implantation site as it does not replicate the dynamic gut environment, nor face the biomechanical and biochemical stimulus it must withstand. Future work could be on implanting at the small intestines to evaluate all facets it must qualify on to translate to clinic. This could also revel insights into anastomosis, biocompatibility, immunomodulation and long-term functionality. The implantation could be carried out in a multi-step manner, omentum implantation to achieve vascularization of the graft and thereby maturation and intestinal implantation for functionality assessment.
- Grow Factor Gradient Delivery
PGS has shown tremendous potential to serve as the biomaterial for intestinal tissue engineering with little to no inflammation, excellent biocompatibility, and tunable biomechanical properties. The scaffold had a limitation of delayed degradation such that it outpaced tissue infiltration and formation, unable to serve as a temporizing device. Albeit it possesses immense advantage of encapsulating various growth factors to achieve a coordinated maturation. These encapsulations could be done in a gradient fashion to obtain a crypt-villus axis. Chemoattractant could be loaded onto the scaffold to better recruit host cells for vascularization, epithelialization and enteric nervous system formation.
- Clinical Translation Challenges
Finally, since the study was conducted in small-animal models, questions about scaling, anastomosis, and long-term function in a clinical setting remain unresolved. These limitations offer valuable direction for future studies to enhance translational potential.
🚧 Overcoming Roadblocks in Intestinal Tissue Engineering
Currently the two major roadblocks in intestinal tissue engineering are achieving nutrient absorption and peristalsis. The first could be improved by creating villi imprints for better maximization of surface area and peristalsis maybe achieved either biologically or with the help of a mechanical device. The group currently have attempted at absorption enhancement by creating the villus structure and recently have also created an implantable, biomimetic, magnetically actuated peristaltic pumping apparatus. The system consists of a magnetic pump surrounding an intestinal graft and a rotating external magnetic field generator that produces peristaltic motion in the graft as the field direction alternates [5]. These approaches when combined could yield a definite fully functional artificial intestine – capable of supporting long-term nutrient assimilation and gastrointestinal flow regulation.
🚀 Final Thoughts: Is a Lab-Grown Gut Becoming Reality?
PGS scaffolds represent a promising starting point, offering biocompatibility, tunable mechanics, and surgical handleability. Yet, without tissue regeneration and function, their clinical use remains aspirational. Future efforts must integrate advanced materials, biomechanical and electrical cues, and bioactive signaling to build not just tissue structures but functioning intestinal organs.
Together, these advances mark a transformative step toward engineering a fully functional, clinically viable artificial intestine—one that doesn’t just replace lost tissue but actively supports regeneration, restores function, and offers new hope to patients with intestinal failure. With continued innovation at the intersection of biomaterials, stem cell biology, and bioactuation, the vision of a lab-grown gut that absorbs, contracts, and regenerates like its natural counterpart moves closer to becoming clinical reality.
If this article excited you, consider liking, sharing, and following our journey at Grow Your Tissues.
References:
Statistics Source:
- Engelstad, H. J., & Danko, M. E. (2020). Short bowel syndrome in an infant. Neoreviews, 21(6), e370-e382.
- Shulhan, J., Dicken, B., Hartling, L., & Larsen, B. M. (2017). Current knowledge of necrotizing enterocolitis in preterm infants and the impact of different types of enteral nutrition products. Advances in nutrition, 8(1), 80-91.
- Grant D, Abu-Elmagd K, Mazariegos G, Vianna R, Langnas A, Mangus R, Farmer DG, Lacaille F, Iyer K and Fishbein T: Intestinal Transplant Registry Report: Global activity and trends. American Journal of Transplantation 15: 210–219, 2014. DOI: 10.1111/ajt.12979
Article of discussion:
- Ladd MR, Costello CM, Gosztyla C, Werts AD, Johnson B, Fulton WB, Martin LY, Redfield EJ, Crawford B, Panaparambil R, Sodhi CP, March JC and Hackam DJ: Development of Intestinal Scaffolds that Mimic Native Mammalian Intestinal Tissue. Tissue Engineering Part A 25: 1225–1241, 2019. DOI: 10.1089/ten.tea.2018.0239.
Supporting article:
- Smith, M. E., May, A., Schwehr, T., Erin, O., Tragesser, C., Scheese, D., … & Krieger, A. (2024). MagnetoStalsis: Generating Peristalsis in an Artificial Bowel for Treatment of Short Bowel Syndrome. Journal of Medical Robotics Research, 9(3-4), 2440006.
Image:
- Costello, C. M., Hongpeng, J., Shaffiey, S., Yu, J., Jain, N. K., Hackam, D., & March, J. C. (2014). Synthetic small intestinal scaffolds for improved studies of intestinal differentiation. Biotechnology and bioengineering, 111(6), 1222-1232.

Leave a comment